

Abstract
Introduction: IgM light chain amyloidosis (AL) is a rare complication of IgM associated disorders, with very limited data on biology and outcomes. Our study compares the clinical characteristics, laboratory findings and outcomes in a large cohort of patients with IgM vs. non-IgM AL to delineate the underlying disease biology of this entity.
Methods: Patients with newly diagnosed AL (2006-15) were identified from a prospectively maintained institutional database and grouped by IgM heavy chain. Bone marrow (BM) morphology was reviewed by an expert hematopathologist (RLK). FISH testing included probes for t(11;14) and trisomies of odd numbered chromosomes. MYD88L265P testing was carried out by allele specific PCR and CXCR4WHIM mutation testing was performed by bridged nucleic acid (BNA)-enhanced Sanger sequencing.
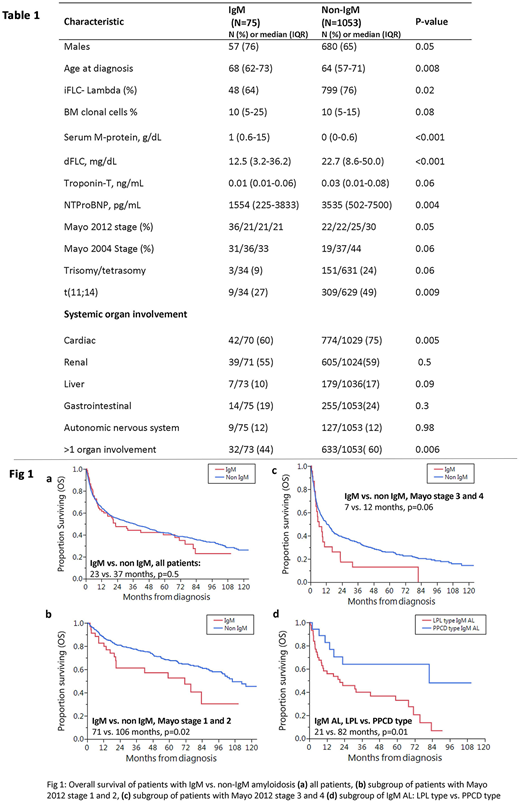
Results: Patients with IgM AL comprised 6.6% (75/1128) of the study cohort. Baseline characteristics are listed in Table 1. IgM AL patients were older and had a higher proportion of males. They had less frequent cardiac involvement (60 vs. 75%) and less frequent involvement of > 1 organ. Light chain burden was lower in this group (dFLC 12.5 vs. 22.7 mg/dL), while there was no difference in BM clonal cell percentage (10% each).
Morphology: BM morphology in 71 patients with IgM AL revealed a pure plasma cell disorder (PPCD type) in 25% (n=18); low-grade B-cell lymphoma (LGBCL) with plasmacytic features (LPL type) in 62% (n=44) [well defined LPL: 38% (n=27), LGBCL with plasmacytic features: 24% (n=17)]; LGBCL, other: 6% (n=4). In the remaining 7%, three patients had other diagnoses and no BM disease in two patients. Median clonal cell % in LPL vs. PPCD type IgM AL was 20% vs. 5%, p<0.001.
Genetics: In patients with IgM AL vs. non-IgM AL, t(11;14) was present in 27% vs. 49%, p=0.009 and trisomies in 9% vs. 24% of patients, p=0.06, respectively. In the IgM AL cohort, MYD88 mutation was seen in 56% (23/41) & CXCR4 mutation in 15% (5/34; S388 type: 3, other: 2) of patients. Importantly, MYD88 and CXCR4 mutations were found only in patients with LPL morphology, while t(11;14) was found only in the PPCD morphology group. There were no patients with both t(11;14) and MYD88 abnormalities (N=26 for both tested). Mutations seen in the LPL vs. PPCD type IgM AL were: MYD88, 88% (22/25) vs. 0% (0/14), p<0.001 and CXCR4, 26% (5/19) vs. 0% (0/13), p=0.02. Conversely, t(11;14) was seen in 0% (0/18) in LPL type vs. 60% (9/15) in PPCD type IgM AL, p <0.001.
Treatment details were known in 63 patients with IgM AL; rituximab-based: 21 (33%), bortezomib/alkylator: 16 (25%), transplant 17 (27%), steroids: one and no treatment: 8 (13%). Treatment in IgM AL LPL type (n=36) was: rituximab based: 16 (44%),bortezomib/alkylator: 5 (14%), transplant: 10 (28%) and none: 5 (14%). In PPCD type [n=17), treatment was rituximab based: 2 (12%), bortezomib/alkylator: 8 (47%), transplant: 7 (41%). At 6 months, very good partial response or better was observed in 26% (10/39) vs. 41% (270/660) of patients with IgM vs. non-IgM AL, p=0.05.
There was no difference in overall survival (OS) when all patients with IgM AL were compared to non-IgM AL (Fig 1a). However, when stratified by early (Stage 1/2) or advanced (stage 3/4) 2012 Mayo stage, patients with IgM AL fared worse (Fig 1b-c). On multivariate analysis, IgM AL was an independent predictor for inferior OS [HR with 95% CI: 1.6 (1.1-2.4), p=0.02] after adjusting for age, Mayo 2012 stage and type of therapy (transplant vs. not). However, when OS was adjusted for 6 month VGPR, there was no difference in OS for IgM AL vs. non IgM AL, p=0.2. In the IgM AL cohort, patients with LPL type IgM AL had inferior OS compared with PPCD type IgM AL, 21 vs. 82 months, p=0.01 (Fig 1d).
Conclusions: Patients with IgM AL have distinct clinical and genetic features, with lower rates of cardiac involvement and a lower frequency of t(11;14) or trisomies compared with non-IgM AL. Even though IgM AL is a rare entity, we were able to delineate two distinct sub-types of IgM AL: LPL type and PPCD type, with implications for therapy and outcomes. Along with unique morphologic findings, presence of MYD88 and CXCR mutations was only seen in LPL type IgM AL and t(11;14) in PPCD type IgM AL. Despite lower cardiac involvement, IgM AL was associated with inferior OS outcomes, likely due to lower response rates, particularly in LPL IgM AL group, which had the lowest OS. Therapeutic approaches targeted towards disease biology to achieve deep responses are needed in this disorder.
Sidana:Janssen: Honoraria. Dispenzieri:Celgene, Takeda, Prothena, Jannsen, Pfizer, Alnylam, GSK: Research Funding. Kapoor:Takeda: Research Funding; Celgene: Research Funding. Lacy:Celgene: Research Funding. Kumar:Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; KITE: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; KITE: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees; Roche: Research Funding; Novartis: Research Funding; Merck: Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Membership on an entity's Board of Directors or advisory committees, Research Funding; Oncopeptides: Membership on an entity's Board of Directors or advisory committees; AbbVie: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding. Gertz:Abbvie: Consultancy; Ionis: Honoraria; spectrum: Consultancy, Honoraria; Apellis: Consultancy; Amgen: Consultancy; Prothena: Honoraria; Teva: Consultancy; Alnylam: Honoraria; celgene: Consultancy; Medscape: Consultancy; janssen: Consultancy; Research to Practice: Consultancy; Physicians Education Resource: Consultancy; annexon: Consultancy.

